| |
|
|
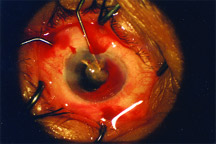
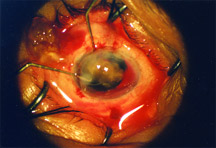
Variation on Kelman’s ‘PAL’ technique uses Sinskey hooks to retrieve the nucleus after posterior capsule tear.
A new bimanual technique, called the “chopstick” technique, causes minimal disturbance to the vitreous, iris, and cornea, according to a recent paper.
This method is used to retrieve a nucleus that is dropping posteriorly after a posterior capsule tear.
The technique was described in a paper co-authored by Harbansh Lal, M.S., and Anita Sethi, F.R.C.S., New Dehli, India. The study was published in the September 2004 issue of the Journal of Cataract and Refractive Surgery.
Another variation on PAL
The chopstick technique is a two-handed method posterior assisted levitation (PAL) for nucleus retrieval that was originally popularized by the late Charles Kelman, M.D., and described in the November 1994 issue of Ophthalmology Times.
With the original PAL technique, a metal sycoldialysis spatula is inserted through a pars plana sclerotomy to lift the descending nucleus, whereas the chopstick technique uses two Sinskey hooks to bring the nucleus into the anterior chamber. One of the Sinskey hooks is inserted from the pars plana to support the nucleus from behind, while the other is introduced via a limbal incision.
Another variation, the Viscoat (sodium hyaluronate 3%; chondroitin sulfate 4%, Alcon, Fort Worth, Texas) PAL, was reported by David F. Chang, M.D., clinical professor, University of California, San Francisco, and Richard Packard, M.D., London, England, in the October 2003 issue of the Journal of Cataract and Refractive Surgery.
In this technique, the viscoelastic cannula is used via the pars plana sclerotomy to levitate the descending nucleus anteriorly. However, prior to elevating the nucleus, Viscoat is first injected beneath the nucleus to support it, and to prevent further descent. Additional small amounts of the dispersive OVD can be injected in order to maneuver and optimally position the nucleus prior to levitating it.
The chopstick technique: A case study
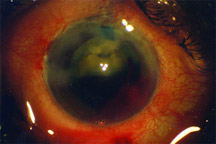
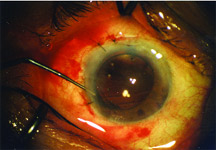
Dr. Sethi and coauthors described the chopstick technique in the case of a 60-year-old man that suffered a torn posterior capsule from a phacoemulsification probe. This injury resulted in an impending dropped nucleus.
Here are the details of the surgery:
• The probe was gently removed while an ophthalmic viscosurgical device (OVD) was injected into the anterior chamber to avoid sudden decompression;
• The continuous curvilinear capsulorhexis was released with a Vannas scissors;
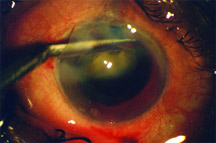
• A 3.0 mm pars plana incision was made behind the limbus, and a Sinskey hook was inserted from the pars plana with the tip pointing upward to support the nucleus from behind;
• A second Sinskey hook was inserted into the anterior chamber from the side-port incision, and the tip was buried in the nucleus. One hook gripped the nucleus while the other one maintained support from behind;
• Gripped between the two instruments, the nucleus was brought out of the capsular bag and into the anterior chamber;
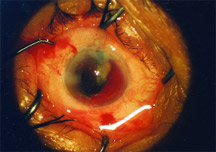
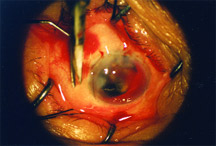
• With posterior support to the nucleus maintained from behind with the first instrument, the incision was enlarged for nucleus removal;
• The second instrument was then removed from above and brought under the nucleus. The pars plana instrument was brought into the chamber and embedded in the top of the nucleus;
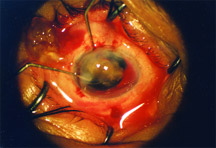
• The nucleus was brought out of the section by holding it in a chopstick grip between the two Sinskey hooks under OVD cover. “The goal was to avoid pressure on the eye and prevent further vitreous loss,” the authors wrote;
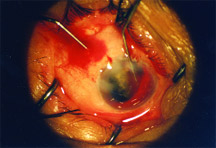
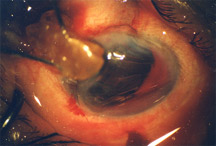
• An anterior vitrectomy with a coaxial cutter was performed through the wound; and
• After vitreous and cortical matters were removed from the anterior chamber, an IOL with a 6.5 mm optic was implanted in the sulcus over the anterior capsule. The incision was then closed with a 10-0 nylon shoelace structure.
Sinskey hooks, spatulas, and viscoelastics
The authors found that retinal trauma could result from using a metal spatula in the nucleus. “We found the Sinskey hook safer and more suitable because it is long enough to stabilize the nucleus and the tip can be easily embedded in the nucleus to provide a good grip,” they wrote.
They added that the use of two Sinskey hooks ensures that the nucleus will not slip and is securely brought out of the enlarged section.
Dr. Chang said that one downside of the chopstick technique is that it requires skillful bimanual control of two instruments amidst the stress of an unexpected complication, where the nucleus can drop at any moment.
“In contrast, dispersive OVD injected beneath the nucleus will immediately stabilize it, allowing the surgeon time to assess the options and to proceed more deliberately,” he said. “If the descending nucleus is located more peripherally, one can aim the OVD behind it, rather than fishing peripherally behind it with a hook. Finally, the chopstick method would be more difficult to employ with multiple small nuclear fragments,” Dr. Chang said.
Caveats
Louis D. “Skip” Nichamin, M.D., medical director, Laurel Eye Clinic, Brookville, Pa., said the chopstick technique is reasonable, but issued a few caveats.
“As with any technique wherein an instrument is placed through the pars plana, one has to be cognizant of where the pars plana incision should be placed,” he said. “It is a somewhat blind maneuver, inserting an instrument back there. But it’s a fairly innocuous procedure overall.”
Dr. Nichamin also cautioned against enlarging the cataract incision and manually extracting the cataract, suggesting instead that the incision be kept small and the phacoemulsification be completed in the anterior chamber.
“Many of us would just as soon leave the lens in the anterior chamber supported with viscoelastic and/or a phaco glide — which is a small lens glide — and keep the small incision, then emulsify the nucleus with phaco in the anterior chamber under generous viscoelastic,” Dr. Nichamin said.
Editors’ note: Dr. Chang is a consultant for AMO. He has no financial interest in any product mentioned. Dr. Nichamin has no financial interests related to his comments.
Contact Information
Chang: 650-948-9123, fax 650-948-0563, dceye@earthlink.net
Lal: 91-11 5851626, fax 91-11 5751002,
harbanshlal@sgrh.com
Nichamin: 814-849-8344, fax 814-849-7130, nichamin@laureleye.com
|