surgical
pearls
Managing Floppy Iris Syndrome
Use of Flomax has been tied to this
complication.
By Jerry Helzner, Senior Editor
David F. Chang, M.D., and John R. Campbell,
M.D., have recently identified a new small-pupil syndrome they've named
Intraoperative Floppy Iris Syndrome (IFIS). They've tied it to use of
Flomax, the most commonly prescribed alpha-adrenergic blocker for the
treatment of benign prostatic hypertrophy (BPH).
IFIS during cataract surgery is characterized
by: iris billowing in response to normal irrigating fluid currents; a
strong tendency toward iris prolapse; and progressive miosis during the
phaco and cortical irrigation/aspiration (I/A) steps.
In this article, we'll provide several pearls
that surgeons should consider when confronted with a potential IFIS case.
|
|
|
|
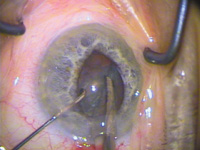
IFIS is characterized by
iris billowing, prolapse to phaco and side port incisions, and
progressive miosis during phaco.
|
|
Mitigating IFIS
Dr. Chang offers the following surgical pearls
for preventing or mitigating IFIS:
"If the pupil dilates poorly preoperatively,
you should specifically ask about prior Flomax use. Even if it has been
stopped for 1 to 2 years, IFIS can still occur, indicating that there must
be some permanent change to the iris dilator muscle. Some urologists
prescribe Flomax for urinary retention symptoms in women, and predictably,
IFIS has been encountered in female Flomax patients.
"It is not clear whether other
nonsubtype-specific alpha-1 blockers cause IFIS. While the IFIS patients
in our two studies were all on Flomax, a few anecdotal reports note IFIS
in patients on Hytrin, Cardura, and Uroxatrol.
"Several features of IFIS increase the risk of
complications for an unsuspecting and uninformed surgeon. First, if the
pupil is small, commonly used mechanical stretching techniques, with or
without partial thickness sphincterotomies, are ineffective in maintaining
an adequate pupil diameter. Furthermore, some IFIS pupils dilate quite
well, or expand well enough following viscoelastic injection to make the
capsulorhexis step quite straightforward. It is not until hydrodissection
and phaco that the problems of IFIS suddenly and unexpectedly
occur.
"We reported increased retrospective posterior
capsule rupture rates with IFIS, and believe that the unanticipated
cascade of iris misbehavior was the likely explanation.
"A number of different approaches have been
tried with varying success. Stopping the Flomax for 1 to 2 weeks seems to
permit wider dilation in some eyes, but doesn't alone prevent IFIS.
"Dr. Sam Masket feels that stronger
cycloplegia, such as with atropine, may help. Dr. Dick Lindstrom feels
that supracapsular phaco is a helpful technique, wherein the prolapsed and
tilted nucleus keeps the pupil from constricting all the way down. Drs.
Bob Osher and Doug Koch rely on Healon5 (see below). "I have found that
the tighter 1.2-mm incisions of bimanual microincisional phaco are of some
help in preventing iris prolapse.
"I believe that all of these strategies work
much better if the iris dilates reasonably well to begin with, and are
less effective if the pupil is already small. In that case, the best
strategy is to employ iris retractors in a diamond configuration as
described by Dr. Tom Oetting. Although this increases the cost and
surgical time, it assures a safe-sized pupil opening throughout the case.
Pupil expansion rings are another option, but can be more difficult to
insert if the chamber is shallow, or the pupil is small."
Using Healon5
To safely and effectively manage the challenges
of IFIS, Robert H. Osher, M.D., uses his slow-motion phaco technique and
Healon5.
In slow-motion phaco, vacuum, aspiration and
infusion are carefully managed. After an initial vacuum of 250 mmHg to
burrow into the lens, vacuum and aspiration rates are kept lower than
normal, which allows a lower infusion rate and fosters stability.
The viscosity and space occupation properties
of Healon5 make it ideal for use with this technique, Dr. Osher says.
"First, viscomydriasis with Healon5 allows me
to create an adequate capsulorhexis without iris prolapsing to the wound,"
he explains.
"During nucleus chopping and removal, not only
does the slow-motion phaco preserve the Healon5 in the anterior chamber,
it deters the floppy iris from 'leaping' into the phaco tip, even though
the pupil may get smaller. I have also learned how to remove cortex
without disturbing the OVD, still keeping the floppy iris from
leaping."
|
|
|
|
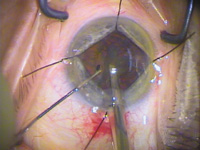
Disposable iris retractors
placed in a diamond configuration in IFIS patient. Subincisional
retractor is placed through a separate stab incision just posterior
to the phaco incision.
|
|
For removal of the Healon5, Dr. Osher places
the I/A tip under the IOL, directs the port toward the single-piece
acrylic IOL, and with several seconds of high vacuum, evacuates the
viscoelastic from the capsular bag. To complete the evacuation, he places
the tip in the anterior chamber with the port toward the cornea.
Before he removes the irrigating tip, he puts
the 27-gauge cannula through the stab incision and holds it against the
optic. He injects Miochol as the I/A tip is being withdrawn.
"This maneuver keeps the chamber from abruptly
shallowing because the Healon5 effectively masks positive pressure," Dr.
Osher says. "The iris prolapse is retarded by the deeper chamber into
which the pupil rapidly constricts from the Miochol."
Dr. Osher has performed phacoemulsification on
approximately a dozen patients with IFIS, and says, "I have not had to
rely on either iris hooks or a mechanical device for pupil dilation."
Multicenter Study Started
"We don't really know whether IFIS will be
associated with a higher rate of cataract surgical complications now that
ophthalmologists can foresee and anticipate the problem," says Dr Chang.
"For this reason, we've started a multicenter prospective study to assess
what the complication rate of IFIS will be, as long as the surgeon is
prepared and able to use alternative pupil management strategies such as
those we describe. We plan to enroll up to 150 consecutive Flomax patients
at 11 sites across the country."