| Currently, the Crystalens (Eyeonics, Inc., Aliso
Viejo, Calif.) is the only Food and Drug
Administration-approved accommodating
intraocular lens. Its clinical results have
been promising, and accommodating IOLs offer several
advantages over other types of IOLs.
Despite
improvements in their design, the latest generation
multifocal IOLs still have significant trade-offs, says David
F. Chang, MD, who is a clinical professor
at the University of California, San Francisco, and in private
practice in Los Altos, Calif. Multifocality
produces significant aberrations and an inherent reduction in
contrast. There will always be halos or ghost images
produced by the secondary focal zone. Finally, a multifocal
lens cannot provide excellent vision across the entire range
of intermediate to near zones. Therefore, accommodating IOLs
offer the promising prospect of better contrast, fewer
aberrations and ghost images, and a better range of
intermediate to near focus.
I. Howard
Fine, MD, agrees. The trend will be toward accommodative
lenses, especially as the technology improves, adds Dr. Fine,
who is a clinical professor, Oregon Health and Sciences
University, and in private practice at Drs. Fine, Hoffman, and
Packer, in Eugene, Ore.
Following
is a look at some of the newest accommodative IOL designs.
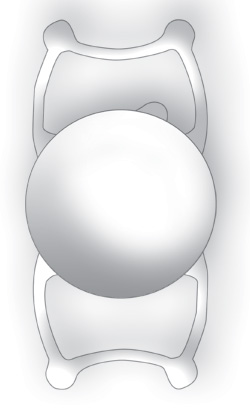
Synchrony
According
to Dr. Chang, who is the medical monitor for the Synchrony IOL
(Visiogen Inc., Irvine, Calif.), this lens is a single piece,
dual-optic accommodating IOL made of the latest-generation
silicone. It features a 5.5-mm high-power anterior optic and a
6-mm negative-power optic. The optics are connected by haptics
that act like springs.
 |
| Figure 1: The Synchrony IOL and
injector. |
The
refractive shift produced by any optic movement is
proportional to the dioptric power of the lens.
Therefore, the anterior moving optic of the Synchrony is
a 32 D (+) lens in order to maximize the near shift produced
by its forward movement. The rear optic is a minus lens that
has varied power in order to achieve the net IOL power
required for emmetropia, he says.
The
design of the Synchrony relies on the Helmholtz
theory of accommodationciliary muscle contraction
reduces zonular tension, allowing the capsular bag to
become lax. This allows the spring-like connecting struts to
push the anterior optic forward. Ultrasound biomicroscopy
imaging has confirmed that the front optic does move enough to
produce the approximately 2.5 D of accommodation measured with
defocus curves, adds Dr. Chang.
Clinical
trials are ongoing in Europe and South America, and the FDA
Phase II trial began in November 2005, with five study sites
in the United States. Ten lenses were implanted in 2005
in the United States, and more than 200 lenses have been
implanted outside the United States.
Ivan
Ossma, MD, MPH, a clinical professor of ophthalmology,
Universidad Industrial de Santander,
Bucaramanga, Colombia, has compiled two-year
follow-up data on 24 eyes implanted with the Synchrony
lens. At three months, 63 percent had uncorrected distance
vision of 20/40 or better, and 100 percent had uncorrected
near visual acuity of 20/40 or better. At six months, 79
percent had 20/40 or better uncorrected distance vision. At
both 12 and 24 months, 83 percent had uncorrected distance
vision of 20/40 or better, and 100 percent had
uncorrected near visual acuity of 20/40 or better. Study
results were reported at the American Academy of Ophthalmology
meeting in Chicago.
Additionally, Burkhard Dick, MD, conducted a
prospective clinical trial on 15 eyes of 12 patients.1 He
performed surgery on all 12 patients, and there were no
intraoperative complications. All eyes have at least six
months of follow-up, and no case of interlenticular
opacification has occurred. He has not seen any serious
complications, and no lenses have been explanted. All
patients were very satisfied with the visual functioning and
achieved accommodation ranges between 0.5 D and 2.5 D, says
Dr. Dick, who is a professor of ophthalmology at Johannes
Gutenberg University, Mainz, Germany.
FlexOptic
The
FlexOptic lens (Advanced Medical Optics) is an
accommodative IOL that conforms to the geometry of the
capsular bag and changes curvature. As the ciliary muscle
constricts, the bag will constrict, and the optic will
actually change its radius of curvature, says Mark Packer,
MD, assistant clinical professor at Oregon Health and Sciences
University, and in private practice at Drs. Fine,
Hoffman, and Packer in Eugene, Ore. Unlike the
Crystalens and the dual-optic lenses, this IOL is not
designed to move axially in the eye. At least in theory,
more accommodation is possible from a change in surface
curvature than from axial movement, even with two
optics.
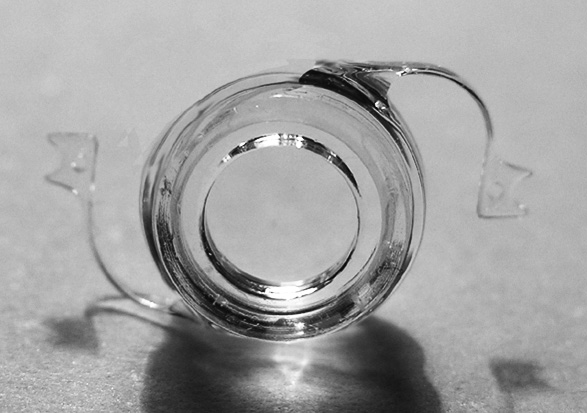
 |
| Figure 2. The TetraFlex lens by
Lenstec. |
Currently,
only benchmark testing has been conducted on the latest
design of this lens.
Smart IOL
The Smart
IOL (Medennium Inc., Irvine, Calif.) is a concept for a
bag-filling IOL that will allow the ciliary muscle to resume
control of lens shape alteration. Filling the bag will
eliminate problems with decentration and edge effects,
according to Dr. Fine.
One
popular concept has been to develop a gel that could fill
the emptied bag and remain flexible, says Dr. Chang.
However, this approach creates many new challenges. How much
gel does one inject? How does one control the net resulting
lens power? How does one seal the capsulotomy, and can a dense
cataract be removed through a micro-capsulorhexis that would
be most compatible with such injectable gel technology?
Finally, how does one produce a precise optical shape with
this method?
The
advantage of the Smart IOL is that the hydrophobic acrylic
lens can be manufactured to precise optical specifications,
including power and anterior and posterior curvature.
However, because of its unique thermoplastic
properties, it can then be reconfigured into a thin rod that
can be implanted through a phaco incision. After implantation,
warming to body temperature causes the shape to transform back
to its original designed configuration, which will completely
fill the capsular bag. One theoretical advantage of this
design is that it is compatible with current phaco methods and
a standard-sized capsulorhexis, according to Dr. Chang.
The Smart
IOL has been implanted into cadaver eyes, but must undergo
further testing before clinical trials can begin.
FluidVision
FluidVision (PowerVision Inc., Belmont,
Calif.) is representative of a new generation of IOLs whose
goal is to produce enormous accommodative rangepossibly
exceeding 10 D, according to Dr. Chang. This is accomplished
through a hydraulically induced shape change that is
controlled by the ciliary muscle.
Fluid is
pushed through tiny hydraulic actuators. As the ciliary body
constricts and the zonules relax, the lens thickens like the
human crystalline lens. Upon relaxation, the zonules become
taut, and the lens becomes thinner. So, through fluid
movement, the lens achieves shape change, which is how we
think the human lens works through the Helmholtz theory, says
Louis D. Nichamin, MD, medical director of the Laurel Eye
Clinic in Brookville, Pa.
Such a
system would be more forgiving of power miscalculation and of
any physiologic or anatomic degradation of its accommodative
power over time, Dr. Chang adds.
The
company has completed a preliminary product design. The next
step will be completion of a 1:1 scale prototype followed by
the first primate implant.
TetraFlex
The
TetraFlex IOL (Lenstec, Inc., St. Petersburg, Fla.) is an
acrylic lens with square-edge technology that was developed by
Robert E. Kellan, MD, assistant professor of ophthalmology at
Boston University and associate ophthalmologist at Tufts
University School of Medicine. It was designed not so much to
use vitreous movement as to use the ciliary zonular capsular
dynamic to ensure maximum forward movement for clear near
vision. It is important to note that all of the theories of
accommodation are merely theories. No one knows the true
mechanism of accommodation, he says.
Sunil
Shah, MD, from the Midland Eye Institute, Solihull, UK, has
assessed both the objective and subjective performance of this
lens, and both studies were presented at the AAO meeting in
Chicago.
The
subjective study included 100 consecutive eyes that underwent
phaco and implantation of the TetraFlex lens. Patients ranged
in age from 40 to 86 years, with a mean age of 71 years.
Patients postoperative spherical refraction was 0.23 ±0.69 D,
and their postoperative cylindrical refraction was 0.83 ±0.48
D. Mean IOL power was 21.5 D, with a range of 19.5 D to 25.5
D. Best-corrected acuity was 0.06 ±0.13 logMAR at distance and
0.58 ±0.20 logMAR at near. Patients subjective amplitude of
accommodation at one month was 3.1 ±1.5 D, with a range of 1 D
to 6.4 D, and their amplitude of accommodation at six months
was 1.7 ±2.2 D, with a range of 1 to 6 D.
The
objective study included 50 patients, and their objective
amplitude of accommodation was 0.4 ±0.6 D, with a range of 0
to 2.3 D.
 |
| Figure 3. The
NuLens IOL. |
Techniques
used in this study to assess the objective accommodation did
not pick up significant changes that would explain the
subjective findings. However, further early work has
demonstrated focal rather than global changes, which are more
in keeping with the subjective findings, Dr. Shah says.
The
TetraFlex has been approved in Europe, Australia, the Middle
East and other markets since early 2003. Approximately
6,000 lenses have been implanted to date. The lens is
currently in FDA clinical trials in the United States, and 138
eyes have been implanted with the lens in this country. Of the
80 cases that have been followed for six months or longer, 48
(60 percent) had 20/40 or better distance corrected near
vision.
Additionally, this IOL effectively caused 94.7
percent of 94 reported cases to be within ±1 D of
emmetropia, and 70.2 percent of cases were
within ±0.5 D at 6 months or later. Target refractions
ranged between emmetropia and 0.25 D.
Of 91
reported cases, 95.6 percent had accommodative amplitudes of
more than 1 D, 69.2 percent could accommodate more than 2 D,
and 19.8 percent could accommodate more than 3 D, according to
Jim Simms, vice-president of Lenstec.
The
company hopes that the TetraFlex will enter the U.S.
market by 2008.
NuLens
NuLens
(NuLens Ltd., Herzliya Pituach, Israel) is composed of a
flexible polymer between two rigid plates, one of which has an
opening. When the plates are compressed, the flexible polymer
bulges through the opening in the front surface, creating a
much more plus-powered lens, explains Dr. Fine, who is a
member of NuLens scientific advisory board.
The lens
is designed to be placed in the ciliary sulcus and promises
between 30 D and 50 D of accommodation. This lens is not a
slam dunk yet, but its very promising, he says. The lens was
developed by Joshua Ben-Nun, MD, who recently published a
feasibility study of this lens.2
The study
was coauthored by Jorge Alio, MD, PhD, and was conducted at
the Vissum-Instituto Oftalmologico de Alicante and Miguel
Hernandez University in Alicante, Spain. A laboratory
lens model was used to assess the feasibility of the concept.
An implantable measuring device was designed and implanted in
monkey eyes to measure the lens action and other parameters.
These measurements were used to build an accommodating IOL
prototype that was then implanted in monkey eyes.
Drs.
Ben-Nun and Alio used pharmacologic agents to achieve ciliary
relaxation and spasm. Additionally, they used ultrasound
biomicroscopy imaging to document the active changes of the
IOL flexible lens curvature as related to the ciliary muscles
status.
They
found that the laboratory model produced more than 50 D of
accommodation, and the ultrasound biomicroscopy imaging
demonstrated changes in lens curvature between 9 D and 53
D.
LiquiLens
LiquiLens
is an accommodative IOL being designed by Vision Solutions
Technologies (Rockville, Md.), according to Dr. Fine. It is a
C-loop lens that contains two immiscible fluids in the center
of the lens. The two fluids will have different refractive
indices. The lens will be filled three quarters of the way
with one of the fluids, and a higher refractive index fluid
will float above that, he says.
The
refractive index in three quarters of the lens is designed for
distance. If patients want to read, they can tilt their heads
down, and gravity will force some of the heavier fluid to flow
along the increasingly lower front surface of the lens. The
result will be a higher refractive index fluid above a lower
refractive index fluid and a more plus-powered lens.
|