OCULAR SURGERY NEWS EUROPE/ASIA-PACIFIC EDITION October 2002
Four strategies help manage posterior capsule rupture with nucleus present
Viscoat PAL, the Viscoat trap, bimanual pars plana vitrectomy and bimanual I&A can prevent dropped lens material.
Michela Cimberle
 SAN FRANCISCO,
U.S.A. Management of vitreous loss and residual lens material should involve
four complementary strategies, according to a surgeon here.
SAN FRANCISCO,
U.S.A. Management of vitreous loss and residual lens material should involve
four complementary strategies, according to a surgeon here.
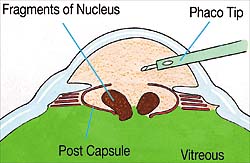
Posterior capsule rupture with nuclear fragments still present in the eye is one of the most stressful complications for the cataract surgeon, said David F. Chang, MD, a clinical professor of ophthalmology at the University of California, San Francisco.
When this happens, you must not only prevent the nucleus from dropping posteriorly, but you must also bring the fragments into the anterior chamber for removal, retrieve the epinucleus and cortex and at the same time preserve as much of the capsule as you can to support the IOL, explained Dr. Chang. Vitreous prolapse further complicates matters, because it is the vitreous that supports the lens fragments after the capsule ruptures. As we lose or excise the vitreous, we lose this remaining support and the lens material suddenly descends.
Dr. Chang said a combination of four sequential strategies can best achieve these four goals.
|
|
Rescuing a dropped nucleus
Bringing a descending nucleus into the safety of the anterior chamber may be difficult, especially if the pupil and capsulorrhexis are small, according to Dr. Chang.
|
|
Any instrument inserted through the phaco wound is approaching the nucleus from the wrong angle. One must avoid the temptation to aspirate a descending nucleus with the phaco tip, Dr. Chang cautioned. Not only will the downward-directed infusion propel the nucleus further away, but aspirating vitreous can create giant retinal tears.
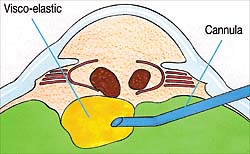
Charles Kelman, MD, first described the posterior assisted levitation (PAL) technique for this situation. Dr. Chang described the PAL technique and subsequent variations.
A metal spatula, inserted through a pars plana sclerotomy, can levitate the nucleus forward. This incision location provides a better angle for getting behind the lens. Richard Packard, MD, then came up with the wonderful idea of using Viscoat [chondroitin sulfate, sodium hyaluronate, Alcon] instead of a spatula for the PAL technique, he said.
First you inject Viscoat behind the nucleus to provide sufficient support, and then with a combination of additional Viscoat injection and manipulation of the cannula tip, you can bring the nucleus up into the anterior chamber through even the smallest capsulorrhexis and the smallest pupil, Dr. Chang continued.
The nucleus can then be removed either by manual extraction through a large incision or by continuing phacoemulsification over a Sheets glide, as originally described by Marc Michelson, MD, he said.
The Viscoat trap
While the Viscoat PAL can bring residual lens fragments and material into the anterior chamber, the next problem arises once vitreous prolapses forward, according to Dr. Chang.
At this point, continued phaco or aspiration becomes dangerous, and a vitrectomy must be initiated, he said.
Surgeons typically insert the vitrectomy tip through the phaco incision at this point with a separate limbal infusion, but Dr. Chang disagrees with this approach.
The phaco incision is too large for the vitrectomy cutter. This causes excessive amounts of vitreous to prolapse alongside the instrument shaft out through the wound, he explained.
This approach also pulls more and more vitreous forward. As the suspended lens remnants are freed, they suddenly drop posteriorly due to the loss of any remaining vitreous support, Dr. Chang said.
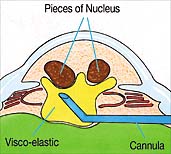
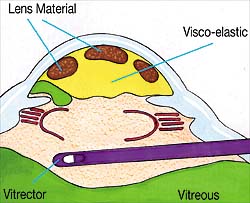
To prevent this, Dr. Chang devised a strategy he calls the Viscoat trap.
Once there is vitreous prolapse, you must stop phaco or irrigation and aspiration. I levitate any lens fragments or material almost right up to the cornea, and then I fill the anterior chamber with Viscoat, Dr. Chang said.
The Viscoat will suspend and trap the fragments as vitreous is subsequently excised, he said. He then performs a bimanual vitrectomy with a self-retaining limbal infusion cannula.
I insert the vitrectomy cutter through the pars plana sclerotomy rather than the phaco incision, he said. By keeping the cutting tip just behind the pupil, I can transect any transpupillary bands of vitreous without aspirating the Viscoat in the anterior chamber. I use Viscoat because its dispersive; it will stay where you put it and resists aspiration by the vitrectomy instrument positioned behind the pupil.
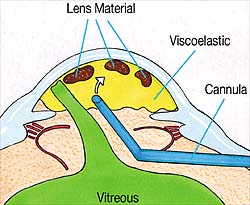
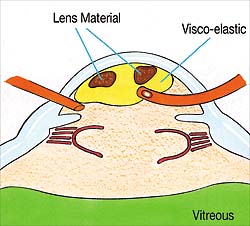
Pars plana bimanual vitrectomy
For the vitrectomy, Dr. Chang uses the same pars plana sclerotomy that was created for the Viscoat PAL maneuver, because it is an appropriately tight incision.
This gives us better fluidics; we dont have vitreous prolapsing through the incision; we do not draw more vitreous into the anterior chamber; and by performing the vitrectomy right behind the pupil, we dont disrupt the vitreous trap in the anterior chamber, Dr. Chang said.
Finally, once the vitreous bands have been cut, Dr. Chang recommends using a bimanual I&A system to remove the remaining cortex and epinucleus.
This is a low-flow system, and the tighter limbal incisions provide more stable fluidics. In addition, thanks to this tight incision, you again avoid having vitreous prolapse alongside the instruments. You have better maneuverability, because the aspirating port can be positioned in the far periphery and kept oriented away from the posterior capsule defect, he explained.
Together, Dr. Chang and Dr. Packard have used the Viscoat PAL technique in eight patients.
In all eight cases we were able to levitate the nucleus and remove it, either by a standard extracapsular cataract extraction (in three cases) or by phacoemulsification (in five cases). We were able to implant posterior chamber IOLs in all in all but one patient, who received an anterior chamber IOL. No patient required any additional vitreoretinal surgery, he said.
For Your Information:
- David F. Chang, MD, can be reached at 762 Altos Oaks Drive, Suite 1, Los Altos, CA 94024, U.S.A.; +(1) 650-948-9123; fax: +(1) 650-948-0563; e-mail: dceye@earthlink.net.