
David F. Chang, MD did not
indicate a financial interest in this report. E-mail:
dceye@earthlink.net
|
San FranciscoQuestioning
patients before cataract surgery about whether they are taking
alpha-1 blockers, such as tamsulosin (Flomax, Boehringer
Ingelheim), has become increasingly important in light of the
observation by David F. Chang, MD, and John R. Campbell, MD,
that the drug, which is used to treat the symptoms of benign
prostatic hyperplasia, can cause intraoperative floppy iris
syndrome (IFIS).
Dr. Chang reported at the
recent American Society of Cataract and Refractive Surgery
annual meeting that the complication rate is acceptably low
when surgeons are forewarned about use of the alpha-blocker.
Dr. Chang is clinical professor of ophthalmology, University
of California, San Francisco, and is in private practice in
Los Altos, CA. Dr. Campbell is in private practice in San
Rafael, CA.
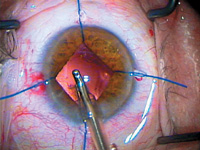
Figure 1 Cortical
irrigation/aspiration in patient with intraoperative
floppy iris syndrome with iris retractors.
|
"When we first presented our
observation of floppy iris syndrome about 1 year ago, one of
the things we highlighted was the higher surgical complication
rate," Dr. Chang said. He demonstrated a case in which the
patient had a well-dilated pupil preoperatively that suddenly
deteriorated into the classic IFIS triad of iris billowing,
iris prolapse, and progressive miosis.
As Dr. Chang had reported
previously, stopping the drug is often ineffective and
pupil-stretching techniques may actually worsen the iris
prolapse. The original paper by Chang and Campbell had
reported a 12.5% incidence of posterior capsular rupture in a
retrospective chart review.
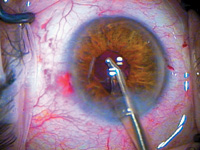
Figure 2 The same patient
following removal of retractors. (Photos courtesy of
David F. Chang, MD)
|
"Four of the IFIS patients in our
series had already undergone prior surgery of their
contralateral eye at another institution. Fifty percent of
these individuals had had posterior capsule rupture and
vitreous loss in their first eye," Dr. Chang noted.
Other surgeons conducting
retrospective chart reviews found high complication rates with
IFIS. Colleague Richard Beller, MD, Napa, CA, found that in
five of his six total cases of posterior capsular rupture
since 2000, the patients had been taking tamsulosin. Likewise,
Bonnie Henderson, MD, affiliated with the Massachusetts Eye
and Ear Institute, Boston, retrospectively reviewed all the
cases in the resident database with a history of tamsulosin
use. The review covered the 2 years immediately prior to the
IFIS report, and five of the seven cases identified had had
posterior capsule rupture.
"This raised the questions
of what to tell our patients taking tamsulosin, what to tell
colleagues in urology about prescribing the drug, and what
would the complication rate be if surgeons knew in advance to
anticipate the IFIS," Dr. Chang explained.
Prospective trial
In light of these
questions, Dr. Chang organized a prospective 10-site U.S.
trial that started in 2005. A total of 167 consecutive
patients undergoing cataract surgery and taking tamsulosin
were enrolled over a 6-month period. Participating surgeons
were asked to use one of four management strategies: 2.3%
sodium hyaluronate (Healon5, Advanced Medical Optics [AMO]),
iris hooks, pupil expansion rings, or atropine drops
administered preoperatively.
"We were not performing a
randomized trial to determine which technique was superior. We
wanted to allow surgeons to do whatever they believed was
appropriateincluding the combination of multiple strategies
in the same case if needed," Dr. Chang explained.
"Most of the procedures,"
Dr. Chang reported, "were performed using either sodium
hyaluronate or iris hooks. About two-thirds of the cases had
mild to moderate nuclear density, and one-third of the nuclei
were dense. Most surgeries were performed using topical
anesthesia and a phaco chop technique."
In addition, the surgeons
performing the surgeries were highly experienced.

