|
EVERY CATARACT SURGEON should have a game plan for when and
how to perform an anterior vitrectomy following posterior
capsule rupture. This article will review the goals, the
indications, and the techniques. Understanding and mentally
rehearsing these strategies will better prepare cataract
surgeons to make correct decisions amidst the stress of an
unexpected complication.
Vitreous Loss after PC Rupture
In
many instances with a torn posterior capsule, it is possible
to avoid rupturing the hyaloid face. The surgeon must avoid
immediately withdrawing the phaco tip upon recognizing a
posterior capsular defect. This abruptly unplugs the incision
and allows the anterior chamber to collapse. The sudden
posterior pressure gradient will rupture an intact hyaloid
face, and vitreous will prolapse to the incision, expanding
the capsular rent in the process.
This undesirable
cascade of events can be avoided by filling the anterior
chamber with viscoelastic prior to removing the phaco tip. As
viscoelastic is injected through the side-port opening, the
surgeon moves from foot pedal position one to zero. Once the
chamber is filled, the posterior capsule cannot bulge forward
as the incision is unplugged. If one resumes
phacoemulsification or cortical cleanup, the same maneuver
must be repeated whenever the instruments are removed.
Managing the Nucleus
Early
recognition of posterior capsule rupture is often the key to
avoiding a dropped nucleus. It is much easier to remove the
nucleus while it remains anterior to the posterior capsule
defect. Because subsequent instrument and fluidic forces
approach the nucleus from above, they will eventually expand
an unrecognized capsular defect enough to allow the nucleus to
sink posteriorly.
One must often rely upon indirect
clues to recognize a posterior capsular defect, because the
iris and the nucleus obscure the zonular and posterior
capsular anatomy. Sudden deepening of the chamber with
momentary expansion of the pupil, the transitory appearance of
a clear red reflex peripherally, and the inability to rotate a
previously mobile nucleus can all indicate capsular or zonular
rupture. More obvious and ominous signs would be excessive
tipping or lateral mobility of the nucleus, or partial
posterior descent of the nucleus.
If the remaining
nucleus or fragments can be elevated into the anterior chamber
with a dispersive viscoelastic, one can insert a trimmed
Sheets glide through the phaco incision to serve as an
artificial posterior capsule, as described by Marc
Michelson.1 The glide can keep lens material from
dropping posteriorly and will shield the phaco tip from
aspirating vitreous from below. The incision should be
slightly widened to accommodate inserting the phaco tip above
the glide. Maneuvers of the phaco tip should be minimized to
avoid simultaneously moving the glide. This is one advantage
of using bimanual microincision phaco instrumentation through
separate 1.2-mm side ports in this situation if the surgeon is
adept at this technique.
The Viscoat PAL
How far the
nucleus initially descends will depend upon the vitreous
anatomy. If the vitreous is very liquefied, the nucleus may
rapidly sink to the retina precluding any response by the
cataract surgeon. Alternatively, the nucleus may partially
descend onto an intact hyaloid face. Such slight posterior
displacement can be very subtle. Finally, if the hyaloid face
is ruptured, the nucleus may tip or partially descend until it
is suspended and supported by formed vitreous. In this
situation, a rescue technique may be possible.
The
worst tactic for recovering a partially descended nucleus is
to try to chase and spear it with the phaco tip. Lacking the
normal capsular barrier, the posteriorly directed irrigation
flow will flush more vitreous forward, expanding the rent and
propelling the nucleus away. Attempting to emulsify or
aspirate the nucleus may ensnare vitreous into the
large-diameter phaco tip. Applying suction and ultrasound
following vitreous incarceration can produce a giant retinal
tear.
The safer alternative is to elevate the nucleus
into the pupillary plane or anterior chamber from below. There
are, however, numerous obstacles to doing this. First, the
pupil or capsulorhexis diameter may be quite small, which may
have predisposed the eye to capsular rupture in the first
place. A small pupil or capsulorhexis can impede elevation of
a large nucleus and make it particularly difficult for a
viscoelastic cannula to maneuver behind it. Prolapsed vitreous
will further hinder such attempts to inject viscoelastic
beneath the nucleus. The nucleus may suddenly sink if these
maneuvers cause further vitreous loss and prolapse.
Charles Kelman popularized the posterior assisted
levitation (PAL) technique in which a metal spatula, inserted
through a pars plana sclerotomy, is used to levitate the
nucleus into the anterior chamber from below. Compared to the
phaco incision, a pars plana sclerotomy provides a much better
instrument angle for getting behind the lens. Richard Packard,
MD, and I subsequently published our results of using Viscoat
(Alcon) and the Viscoat cannula to support and levitate the
nucleusthe so-called Viscoat PAL
technique.2
After opening the conjunctiva
and applying light cautery, a disposable microvitreoretinal
(MVR) blade (Alcon, Katena) is used to make a pars plana
sclerotomy located 3.5-mm behind the limbus. An oblique
quadrant should be selected. The Viscoat cannula is then
advanced and aimed behind the nucleus under direct
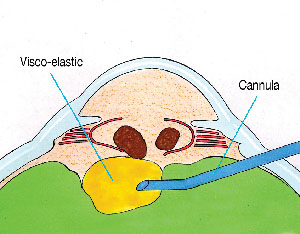
visualization. The first step is to inject a bolus of
dispersive viscoelastic behind the nucleus to provide
immediate supplemental support (See Figure
1). Periodic palpation of the globe confirms that
overinflation has not occurred.
|
|
| Figure 1. Viscoat is injected
via a pars plana sclerotomy behind the descending
nuclear fragments to provide immediate supplemental
support. |
If
the nucleus is subluxated laterally, directing viscoelastic
toward the region beneath it will often buoy the nucleus
toward a more central position. This is preferable to blindly
probing with a metal spatula. One should not attempt to float
the nucleus into the anterior chamber using a massive infusion
of viscoelastic alone. Unlike using liquid perfluorocarbon in
a vitrectomized cavity, an excessive injection of viscoelastic
may overinflate the globe and cause vitreous expulsion through
the sclerotomy.
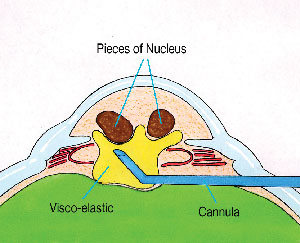
Instead, the cannula tip itself should
be used to mechanically prop and levitate the nucleus into the
anterior chamber (See Figure 2). Small
aliquots of additional viscoelastic can be injected to help in
the elevation and maneuvering of the nucleus. A small
capsulorhexis or pupil will stretch to accommodate the
levitation of a greater-diameter nucleus.
|
|
| Figure 2. The Viscoat cannula
is used to carefully lift the fragments into the
anterior
chamber. |
Using
dispersive viscoelastic to first support and reposition the
nucleus prior to definitive manual levitation is the major
advantage of the Viscoat PAL variation. Because there is no
aspiration involved, these PAL maneuvers should minimize
iatrogenic vitreous traction and reduce the chance of touching
the retina with a metal spatula tip. Although Vitrax (AMO) is
another acceptable dispersive agent, the smaller gauge cannula
of the Viscoat syringe makes it the preferred choice for this
technique.
Once a fragment descends into the mid or
posterior vitreous cavity, it is dangerous to blindly fish for
it with any instrument. One should abandon the dropped nucleus
and concentrate on removing the residual epinucleus and
cortex, while preserving as much capsular support as possible.
A thorough anterior vitrectomy must be performed prior to
inserting the IOL. Because the vitreoretinal surgeon will
later use a three-port fragmatome and vitrectomy technique to
remove any retained nucleus, it is preferable to insert an IOL
through the cataract incision during the initial surgery, if
possible.
The Viscoat Trap
Any
residual nucleus retrieved with the Viscoat PAL technique can
be removed using either of two techniquesresuming phaco over
a Sheets glide or converting to a large incision manual
extracapsular cataract extraction. At some point during this
sequence, the phaco or irrigation-aspiration (I-A) tip may
ensnare prolapsing vitreous. To avoid vitreous traction, the
surgeon must stop to perform an anterior vitrectomy, before
extraction of the remaining lens material can be
resumed.
The most common practice is to place a
separate self-retaining irrigating cannula though a limbal
paracentesis and to insert the vitrectomy probe through the
phaco incision. However, there are multiple drawbacks to this
approach. First, the phaco incision is too large for the
sleeveless vitrectomy instrument. This leaking incision
provides poor chamber stability and allows both irrigation
fluid and vitreous to prolapse externally alongside the
vitrector shaft. Second, performing the vitrectomy in the
anterior chamber will tend to draw more posteriorly located
vitreous forward. Finally, as more and more vitreous exits the
eye through either the cutting instrument or the incision, the
residual lens material that it was supporting will sink down
toward the retina. It bears repeating that once the posterior
capsule is open, it is the vitreous that is preventing the
remaining nucleus and epinucleus from descending.
I
have proposed a strategy, called the Viscoat Trap, which,
when combined with a pars plana anterior vitrectomy, can
prevent this undesirable chain of events.3,4 The
first step is to use a dispersive viscoelastic, such as
Viscoat or Vitrax, to levitate any mobile lens fragments up
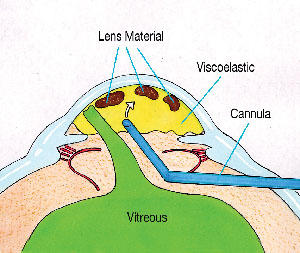
toward the cornea. Next, completely fill the anterior chamber
with viscoelastic. Even though vitreous has already prolapsed
forward, injecting viscoelastic should not exert traction on
the retina. The dispersive viscoelastic can now support and
trap the residual lens material in the anterior chamber as the
vitreous is excised from below (See Figure
3).
|
|
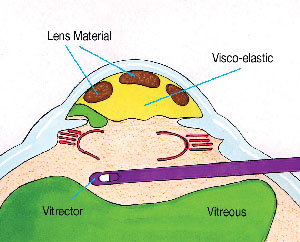
| Figure 3. Following anterior
vitreous prolapse, the residual lens fragments are
elevated toward the cornea, where they are trapped by
filling the anterior chamber with
Viscoat. |
The Viscoat Trap is so named because of the need to
employ a dispersive viscoelastic. To effectively trap lens
material, the viscoelastic should be maximally retentive, so
that it is less easily burped out of the eye through
incisional manipulation. In addition, dispersive agents, such
as Viscoat, better resist aspiration by a nearby I-A or
vitrectomy port. Finally, the smaller size and molecular
weight of dispersive agents makes a prolonged and protracted
pressure spike less likely when small amounts are
retained.5,6
Bimanual Anterior
Vitrectomy
As with the Viscoat PAL, the pars
plana sclerotomy is made 3.5-mm posterior to the limbus. A
disposable #19 MVR blade will create an adequately sized
opening for most anterior vitrectomy cutters and should be
advanced until it is visualized through the pupil. It is
possible to perform this step under topical anesthesia
alone.
A self-retaining irrigating cannula is placed
through a limbal paracentesis and is angled toward the pupil.
As described by Scott Burk, Md, PhD, staining prolapsed
vitreous with a triamcinolone suspension to improve visibility
is an option.7 The sleeveless vitrectomy shaft is inserted
through the pars plana sclerotomy until the tip can be
visualized in the retro-pupillary space. If it does not pass
through the incision easily, it is important to slightly
enlarge the opening rather than to force the
entry.
Using low flow and vacuum settings, and as high
a cutting rate as possible to minimize vitreous traction, a
thorough anterior vitrectomy is performed. One should focus
posteriorly enough with the microscope to keep the tip under
direct visualization at all times. One should attempt to keep
the vitrectomy tip behind the pupil if possible. While any
transpupillary bands of vitreous will still be severed, this
will avoid removing the dispersive viscoelastic that fills the
anterior chamber (See Figure
4).
|
|
| Figure 4. The sleeveless
vitrectomy cutter is introduced via a pars plana
sclerotomy and is kept behind the plane of the
capsulorhexis and pupil. This severs the transpupillary
bands, but keeps the vitrectomy separated from the
partitioned anterior chamber. The self-retaining
infusion cannula (not shown) is placed through a limbal
stab
incision. |
When properly performed, one will see that the anteriorly
trapped lens fragments remain immobilized as the vitrectomy is
being carried out from below. This is because two separate
chambers have been formed by the viscoelastic partition, such
that the anterior chamber is isolated from the vitrectomized
posterior chamber.
The pars plana sclerotomy is an
underused option when performing an anterior vitrectomy. The
principles of anterior vitrectomy technique are the same: one
must not aspirate vitreous without cutting it; one should keep
the vitrectomy tip under direct microscopic visualization; and
one should not attempt to retrieve lens material that is in
the posterior vitreous cavity.
The main advantage is
that using a properly sized sclerotomy will decrease
incisional leak and vitreous prolapse and should provide a
better fluidic seal. Unlike with a limbal incision, the
vitrector need not traverse the anterior chamber and disrupt
the Viscoat partition, and it will not draw more vitreous
forward into the anterior chamber. Performing the vitrectomy
posterior to the pupil and the plane of the capsulorhexis also
decreases the chance of inadvertently cutting either
structure. If the capsulorhexis is preserved, a foldable
posterior chamber IOL may still be implanted in the ciliary
sulcus. The sclerotomy can be closed with an interrupted 8-0
Vicryl suture.
Following the retro-pupillary anterior
vitrectomy, one can resume aspiration of the remaining cortex
or epinucleus trapped in the Viscoat-filled anterior chamber.
Bimanual I-A instrumentation is ideal for epinuclear and
cortical extraction once the capsule or zonules have ruptured.
One should attempt to work in slow motion by lowering the
irrigation bottle and decreasing the aspiration flow and
vacuum settings. If the aspirating ports become entangled with
vitreous again, one can repeat the Viscoat Trap maneuver
followed by additional pars plana anterior vitrectomy.
Bimanual cortical I-A can then be resumed.
Cautious
adherence to these principles may help surgeons to reduce the
chance of dropping the nucleus following posterior capsular
rupture. However, there is a potentially fine line dividing
maneuvers that are reasonable and safe from those that are
overly aggressive or dangerous. Cataract surgeons must be
honest in assessing their own level of comfort and expertise.
Timely surgical management of a dropped nucleus by a
vitreoretinal surgeon at a later date is always preferable to
overstepping this fine line.8
Dr. Chang is a clinical professor at the University of
California, San Francisco, and is in private practice in Los
Altos, Calif. He has no financial interest in any product or
instrument mentioned in this article.
1. Michelson MA. Use of a Sheets glide as a
pseudoposterior capsule in phacoemulsification complicated by
posterior capsule rupture. Eur J Implant Surg
1993;570-572.
2. Chang DF, Packard RB. Posterior assisted
levitation for nucleus retrieval using Viscoat after posterior
capsule rupture. J Cataract Refract Surg
2003;29:1860-1865.
3. Chang DF. Managing residual lens
material after posterior capsule rupture. Techniques in
Ophthalmology 2003;1(4):201-206.
4. Chang DF. Strategies
for managing posterior capsular rupture. In Phaco Chop:
Mastering Techniques, Optimizing Technology, and Avoiding
Complications. Thorofare, NJ: Slack Inc., 2004.
5. Burke S,
Sugar J, Farber MD. Comparison of the effects of two
viscoelastic agents, Healon and Viscoat, on postoperative
intraocular pressure after penetrating keratoplasty.
Ophthalmic Surg. 1990;21:821-826.
6. Probst LE, Hakim OJ,
Nichols BD. Phacoemulsification with aspirated or retained
Viscoat. J Cataract Refract Surg 1994;20:145-149.
7. Burk
SE, Da Mata AP, Snyder ME, et al. Visualizing vitreous using
Kenalog suspension. J Cataract Refract Surg
2003;29:645-651.
8. Scott IU, Flynn HW Jr., Smiddy WE, et
al. Clinical features and outcomes of pars plana vitrectomy in
patients with retained lens fragments. Ophthalmology
2003;110:1567-1572.
(See also: New PAL method may save difficult
cataract cases. Ophthalmology Times 1994;19:51).
|